Several plaintiff firms cite the projected lifetime healthcare cost for
patients having a lower extremity amputation as a one-size-fits-all figure of $509,275, while others argue for even larger damage awards based on testimony from life care planners. Both approaches tend to overstate the projections of long-term costs by relying on inappropriate
assumptions and not accounting for the time value of money.
A more accurate projection of long-term costs based on a particular patient’s life expectancy can be obtained according to a methodology developed by medical and business school professors at the University of Michigan who attempted to inform surgeons deciding whether to salvage or amputate lower extremities.1 To guide their treatment decisions, Chung et al. performed an objective analysis of cost data collected from the landmark Lower Extremity Assessment Project
(LEAP) to compare the total costs associated with lower-limb amputation versus the total costs associated with lower-limb salvage.2
In this article, we discuss these cost projections and provide an updated version of Chung’s projections adjusted to today’s dollars. We also discuss other components of damages that plaintiffs commonly assert in litigation involving the amputation of a lower extremity.
Background statistics
Amputations are common in the United States. Nearly 2 million Americans live with limb loss, and approximately 185,000 amputations occur in the U.S. each year.3 The primary medical reasons for lower extremity amputations within this country continue to remain constant
with approximately 54% due to vascular disease (including advanced diabetes, and peripheral arterial disease), 45% due to trauma, and the remaining 1% due to cancer.4
Mortality rates for patients with lower extremity amputations depend on the reason for the amputation. The survival rate for patients who require lower extremity amputations because of trauma is comparable to the general population.5 However, nearly half of the patients that require a lower extremity amputation due to vascular disease die within five years.6
With advances in microvascular and external fixation techniques, orthopedic surgeons face difficult decisions about whether to amputate or to attempt to salvage severely injured lower extremities. LEAP, which is funded by the National Institutes of Health, sought to inform many of the questions surrounding these decisions. A prospective multicenter study, LEAP is the largest primary analysis of limb-threatening injuries. Numerous publications have resulted from LEAP.
There is no data in the orthopedic trauma literature that compares with the LEAP study in terms of the breadth of the data recorded or the number of patients enrolled.7 One of the numerous factors evaluated in this study was an attempt to quantify the long-term cost of care for a
patient with a lower limb amputation. Although LEAP included patients with above-the-knee and below-the-knee amputations, no differences in long-term costs were identified.
Costs involved in lower limb amputation
Plaintiff firms tend to identify three categories of alleged damages associated with a lower extremity amputation:
1. long-term healthcare costs;
2. lost wages; and
3. the cost of future residence in assisted living or nursing home facilities.
Long-term healthcare cost projections: Several plaintiff firms cite the projected lifetime healthcare cost for patients undergoing a lower
extremity amputation as $509,275. This assertion appears to stem from an earlier paper analyzing data from LEAP that projected lifetime costs for amputation patients to be $509,275.8 However, that figure is flawed because it did not account for the time value of money and only
represented a single scenario. This was because assumptions included 42.8 years of remaining life and a frequency of prosthetic purchase once every 2.3 years.
In the 2009 study, Chung took the LEAP data and applied discounting after year 2 to account for the time value of money. Under the time value of money concept, a dollar today is worth more than a dollar next year. Discounting determines how much a series of cashflows in the future is worth as a lump-sum payment today, and it “is an essential practice when alternative interventions have different costs occurring at different times over the remaining life of the patient,” according to Chung.9
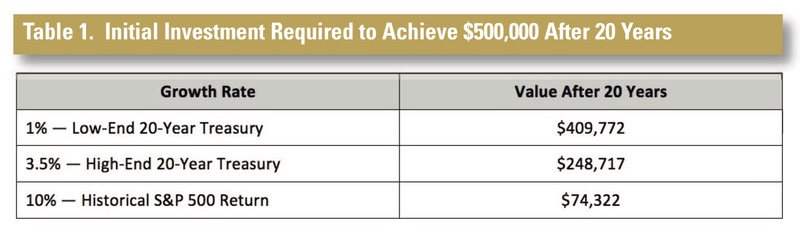
Studies that do not account for the time value of money are likely to overstate the amount of long-term expenses that Chung has alleged in his research. As the authors noted, their use of a risk-free rate leads to a “conservative estimate of the effects of
discounting.”10 If, for example, the authors had applied the average historical rate of return for the S&P 500, the projections would be substantially reduced.
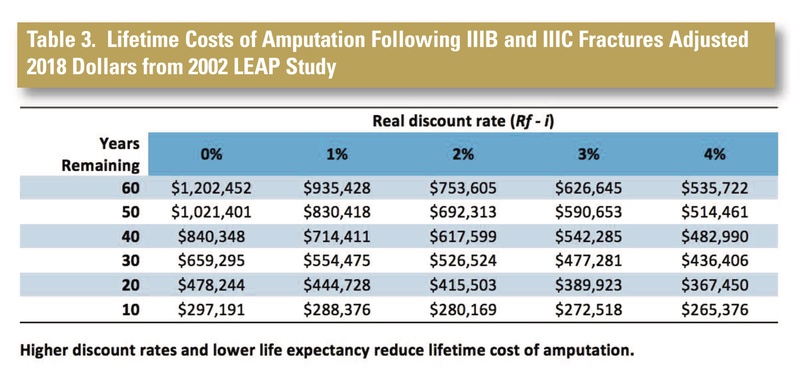
Based on their analyses, the authors presented Table 2 to show several possible lifetime cost projections for a discount rate ranging from 0-4% and life expectancies ranging from 10-60 years. Understanding that LEAP used 2002 cost dollars, we adjusted the costs to reflect 2018 medical cost dollars by using the U.S. Bureau of Labor Statistics. (See Table 3.) The revised 2018 cost figures are significantly higher than 2002. For example, adjusting 2002’s 40-year remaining lifetime costs with discounted rates at 2% to 2018 dollars, increases the estimate
from $349,619 to $617,599. This represents an increase of 77%.
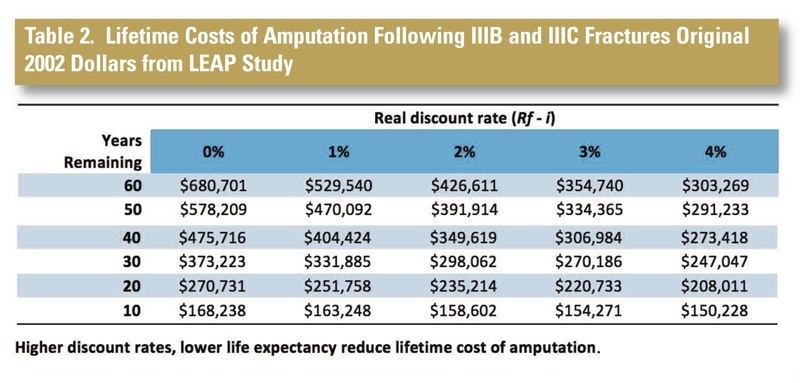
As these tables illustrate, the patient’s life expectancy has a substantial impact on the long-term cost. The discount rate also has a substantial effect on the amount of a lump-sum payment, and the rates selected by the authors (ranging from 0-4%) provide a conservative projection of the discounting effect by using a risk-free rate.
Return to work and lost wages: The appropriate measure of damages for lost wages is fact dependent, but there is scientific literature to inform projections. An in-depth analysis by Dr. Saddawi-Konefka involved the review of 1,947 articles and 28 observational studies involving the comparison of outcomes for patients suffering acute trauma with primary amputation versus limb salvage.11 The mechanisms of injury encompassed by the review included motorcycle accidents, pedestrian accidents, agricultural accidents, falls, gunshots, sports injuries, etc. Notably, the authors found that 73% of patients who required amputation returned to work after an average delay of 14 months.
A 2021 review published by Schade et al. reached similar conclusions in the context of open tibia fractures based on a review of 1,204 studies.12 The review included 17,073 patients, and the most common mechanisms of injury were road traffic injuries, work-related injuries, and falls from height. The authors determined that 89% of the patients were working pre-injury. Most of the patients returned to work after a mean absenteeism of 14 months. Specifically, after injury, 60% continued their prior work, 17% were partially working or changed work, and unemployment among the patients went from 11% to 22%. The mean time to return to work was 14 months.13
Alleged damages for use of long-term care facilities: Plaintiffs may also assert the cost of a long-term care facility such as nursing home or assisted living facility in their damages calculations. However, our review of the literature does not indicate that patients with amputations due to trauma enter assisted living or nursing home facilities more frequently
than the general population. Without any such data, requests for the cost of long-term care facilities are speculative and not supported.
In the final analysis, data from LEAP indicated that many of the patients sustaining severe extremity trauma tend have a great number of social, economic, and personal disadvantages
compared to the general population prior to their injury. Functional outcomes and quality of life outcomes appear to be related to preexisting factors rather than to interventions provided by the healthcare system, regardless of whether the patient underwent amputation or salvage.14
A final word
The amount of long-term costs associated with lower extremity amputations is a common issue in personal injury litigation. Dr. Chung’s methodology provides a fair estimate of those costs based on the patient’s life expectancy, and this article has updated those projections to today’s
dollars.
References
1. “Kevin C. Chung, MD, MS, Daniel Saddawi-Konefka, Steven C. Hasse and Gautam
Kaul, “A Cost-Utility Analysis of Amputation versus Salvage for Gustilo IIIB and IIC
Open Tibial Fractures, Plastic Reconstructive Surgery, December 2009,
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2788746/. <br>
2. Ibid.
<br>
3. “Limb Loss and Limb Differences: Facts, Statistics & Resources,” The Hanger
Clinic, April 30, 2021, https://hangerclinic.com/blog/prosthetics/limb-loss-andlimb-
difference-facts-statistics-resources/.
<br>
4. “Kevin C. Chung, MD, MS, Daniel Saddawi-Konefka, Steven C. Hasse and Gautam
Kaul, “A Cost-Utility Analysis of Amputation versus Salvage for Gustilo IIIB and IIC
Open Tibial Fractures, Plastic Reconstructive Surgery, December 2009,
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2788746/.
<br>
5. Ibid.
<br>
6. Ibid.
<br>
7. Ibid.
<br>
8. Ibid.
<br>
9. Ibid. √
10. Ibid.
<br>
11. Schade et al., “The economic burden of open tibia fractures: A systematic
review.” Injury, Vol. 52, Iss. 6, pp. 1251-1259, Feb. 13, 2021.
<br>
12. Schade et al., “The economic burden of open tibia fractures: A systematic
review.” Injury, Vol. 52, Iss. 6, pp. 1251-1259, Feb. 13, 2021.
<br>
13. Schade et al., The economic burden of open tibia fractures: A systematic review.
INJURY, Vol. 52, Iss. 6, pp. 1251-1259 (Feb. 13, 2021).
<br>
14. “Kevin C. Chung, MD, MS, Daniel Saddawi-Konefka, Steven C. Hasse and
Gautam Kaul, “A Cost-Utility Analysis of Amputation versus Salvage for Gustilo IIIB
and IIC Open Tibial Fractures, Plastic Reconstructive Surgery, December 2009,
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2788746/.
Table 1. Initial Investment Required to Achieve $500,000 After 20 Years
Table 2. Lifetime Costs of Amputation Following IIIB and IIIC Fractures Original 2002 Dollars from LEAP Study
Table 3. Lifetime Costs of Amputation Following IIIB and IIIC Fractures Adjusted 2018 Dollars from 2002 LEAP Study